









For more than a decade, advocates have asked women to let us know if they have “dense” breasts. This not only increases the risk of cancer, but also makes tumors difficult to detect on mammograms. Finally, last month, following a long-awaited U.S. Food and Drug Administration ruling, after giving a patient a mammogram, breast imaging centers will inform patients about their breast density and the risks associated with it, and additional imaging tests can help detect cancer. It was decided that we should inform you of the possibility. Mammography may have been overlooked.
Breasts are considered dense if they consist of more glandular and connective tissue than fat. Radiologists classify breast density into four categories: A, B, C, and D. increase. These range from very fatty to very dense, with many combinations in between. Women in categories C and D (about half of all women) are considered to have dense breasts under FDA guidelines. Only 10% are D only.
Category D women have a 2- to 4-fold increased risk of developing cancer, independent of other risk factors. By some estimates, it’s more likely. Considering density alone, Category C women have about average risk. Women who are transgender and taking feminizing hormones may also have denser breasts and may be slightly more likely to develop breast cancer. , breast density is generally not considered a risk factor in such cases. We recommend that transgender men who have not undergone breast reconstruction surgery follow the same screening protocols as women.
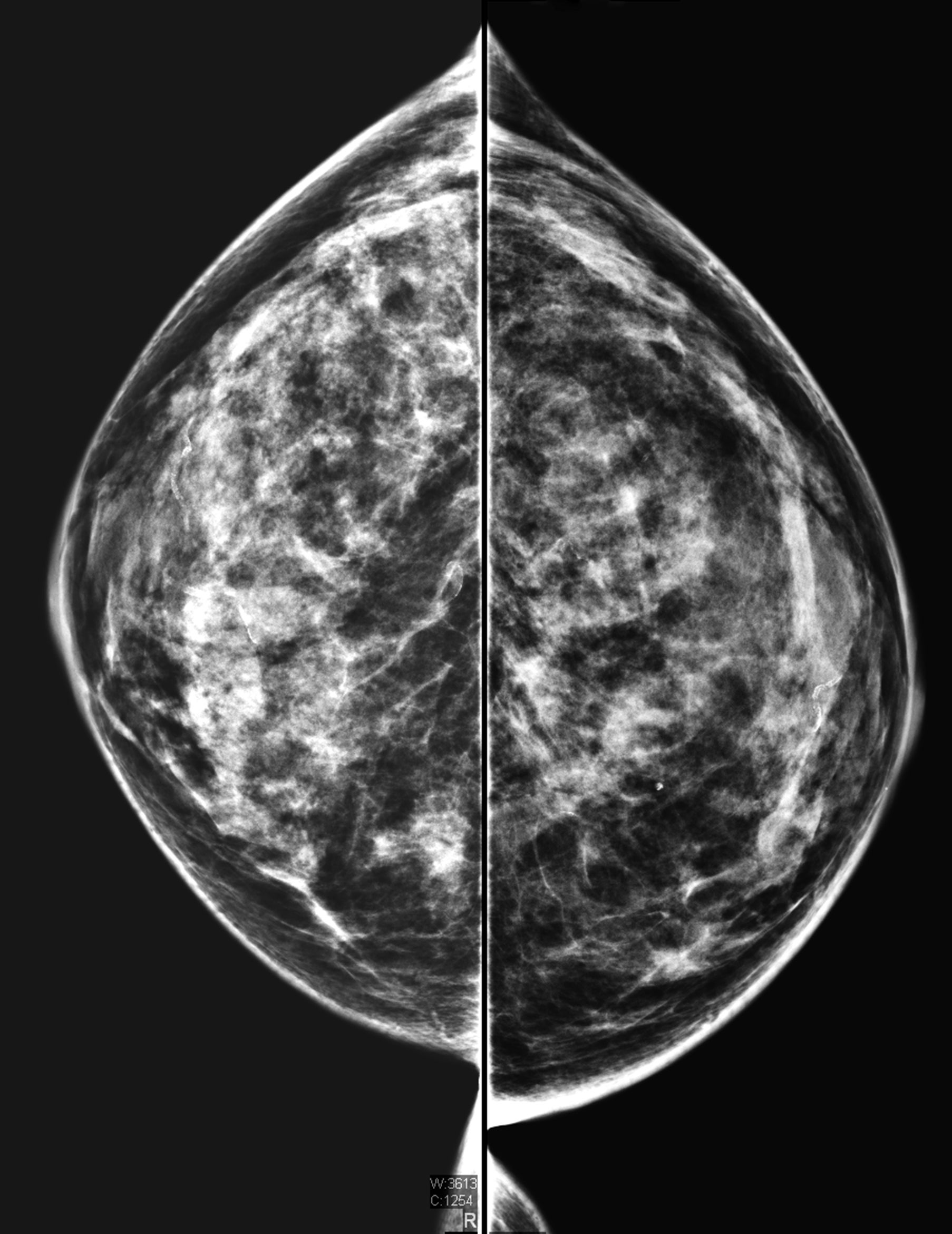
Women with dense breasts can develop cancers that don’t show up on a mammogram. On mammograms, both dense breast tissue and tumors appear white, which can hide cancer. White tumors are more visible in gray-looking adipose tissue.
Advocates and doctors say the FDA’s mandate will help cancers be detected earlier and more often. However, it is not so easy for an individual to determine whether additional screening is necessary and how much benefit can be gained from it. , warns that other factors that influence cancer risk will be downplayed and that additional screening will lead to a higher rate of false positives.
Mammograms miss about 50% of cancers in women with dense breasts. Ultrasound and magnetic resonance imaging (MRI) scans have been shown to detect cancer more effectively than mammography alone. However, due to the high cost and limited availability of MRI and debate about the benefits of additional screening for women with dense breasts, the test is not standardized in the United States. Very dense breasts should have MRI screening every 2-4 years if possible.
Thirty-eight states currently have laws that require providers to be informed of breast density, but the degree of patient education they provide varies. FDA’s mandate establishes consistent language for patient notification. Mammography facilities must be compliant by September 2024. Only half of state laws on breast density notification refer to discussing supplemental screening with a doctor, and all state laws warn patients that dense breast tissue can lead to the development of breast cancer. We’re not asking you to let us know. These discrepancies put women at risk, says Joan Pushkin, a national advocate for breast density notifications. and was later discovered on ultrasound.
“Every state that enacts its own ‘notice’ law adds a new version to the mix.. This creates an unfairness in the actionable information patients receive based on where they live,” he said. Pushkin says. “We need a national reporting standard to ensure consistency from state to state.”
know the risks
The FDA does not specifically recommend additional screening for women with dense breasts, said FDA Chief Medical Officer Hilary Marston. However, the new rule advises physicians and patients to consider breast density along with other cancer risk factors when deciding whether additional screening is necessary. We’re not regulating behavior, and the really necessary follow-up conversation that we’ve set in this rule, especially in this area, is the clinician-patient conversation,” says Marston. “And the details of the patient’s case must be taken into account.”
To determine a person’s cancer risk, doctors incorporate features such as breast density and family history into standard models. Many of them are available online. According to American Cancer Society guidelines, anyone these models determine has at least a 20% lifetime risk of developing breast cancer should have her MRI in addition to a mammogram and benefit from early screening. There is also a possibility. For the model to work most effectively, women should also undergo genetic testing so that health care providers can input genetic abnormalities that increase cancer risk.
Women with very dense breast tissue and no other risk factors probably reach a risk marker of 20% based on density alone, says a professor of radiology at the University of Pittsburgh School of Medicine, advocated in partnership with Pushkin. says Wendie Berg.Women with dense breasts, but not in the highest category “probably [have] If you have other cancer-causing risk factors, your lifetime risk is over 20%,” Berg said.
However, because a minority of women are considered at high risk based on breast density alone, many physicians believe breast density notification methods have so far ignored other risk factors that are important for all women. warned, write Jennifer Haas and Celia, now of Massachusetts General Hospital.Kaplan of the University of California, San Francisco, in a 2015 paper JAMA Internal Medicine.
“Such laws also do not address other important risk factors for breast cancer, such as age and family history of breast or ovarian cancer. BRCA and other genetic alterations, or a previous breast biopsy,” Haas and Kaplan wrote. yeah.”
Also, the radiologist’s determination of breast density is somewhat subjective. If radiologists fear liability for not reporting density, this may lead them to overreport it, and “can order additional screenings… so breast It limits the validity of density assessments,” added Haas and Kaplan.
But advances over the past decade in both image processing and software that classify densities could help reduce variability in assessments, the FDA writes in the new rule. “The potential variability in density assessment does not outweigh the importance of communicating breast density to patients and their healthcare providers.” “Certainly, we knew there could be this masking effect that would make the cancer more difficult to identify on a mammogram, but it became clearer over time.” What we found was that it was an independent risk factor,” she adds.
test selection
Additional screening for people with dense breast tissue has been proven to detect far more cancers than mammography alone, but it can also result in many false-positive biopsies. This has led to significant backlash against breast density laws.
In a Berg-led study of more than 2,800 women with dense breast tissue and high risk of cancer, adding ultrasound to mammography increased cancer detection by 55%. Using mammography alone, the researchers found 7.6 cancers in hers per 1,000. Ultrasound added 4.2 per 1,000 of hers. In a follow-up study by Berg and her colleagues, MRI then detected 14.7 more cases per 1,000 people, 25% more cancer cases for her than mammography and ultrasound combined.
However, because benign masses are often suspected on ultrasound, [after ultrasound] It turned out to be cancer,” Berg says. “This is a lot of extra testing other than cancer, and it’s always been one of his criticisms of ultrasound.”
MRI combined with mammography is usually the most effective screening protocol for women with dense breasts because MRI is so accurate and has fewer false positives than ultrasound, says Berg. does not completely eliminate the risk of false positives, she adds. Several studies of her MRI screening for people with dense breasts have reported false-positive rates of 52-97 per 1,000.
Regardless of the type of screening chosen, many insurance companies will not subsidize additional testing for women who do not meet the 20% lifetime breast cancer risk threshold. Also, many women may choose to decline her MRI due to claustrophobia or other reasons. Berg’s survey found that 42% of those offered her free MRI screening declined her.
Improvements in mammography may make tests more effective in detecting cancer in dense breasts. Contrast-enhanced mammography, in which intravenously injected dye enhances areas seen on mammographic images, has been shown to be nearly as effective as MRI. However, the test is now primarily used to evaluate known cancer cases. A drawback of contrast-enhanced mammography is the risk of allergic reactions to dyes.
“because it’s attractive [unlike MRI machines] There are no tunnels and you can do it with existing equipment, usually just a software upgrade,” says Berg. “Furthermore, contrast-enhanced mammography could be much more widely available and possibly much cheaper than MRI. [dye] It’s cheap. “
Berg hopes the FDA mandate will lead to an open discussion between dense breast patients and their physicians about how to determine individual breast cancer risk and select the best screening.
“I think we need education [women] about the risk of false positives,” she says. “I think decisions should be shared with their doctors, but women should have the information they need to make that decision,” she said.